Our goal is to support measurable change in mental health and wellbeing services, through a collaborative and evidence-based approach. Our clients tell us they need good visibility and value extra support to go from A to B.
Our visibility tools expose the nature of a mental health provider's operating model, with drill down to individual service user journeys. This allows us to confidently identify high impact flow and service model interventions.
Data needs to be triangulated with frontline process observation and staff interviews. This establishes a firm understanding of status quo and supports change consensus build.
Our analysts provide the actionable insights and reporting to preserve a focus on high impact interventions.
Client Testimonials
The VOT team have a long record of client success.
"We are really impressed with the pace at which you have got everyone on board & engaged in this work" "we could not have achieved this transformation without [you]"
West London Trust
Julia Renton, Clinical Director
"Great to take part in the Sheffield Health and Social Care NHS FT Home Treatment away day. The team's response to the fabulous data collated by VOT Health showed the way in which they could better support the right service users to be treated close to home as part of the Home First programme"
Sheffield Health Partnership
Helen Crimlisk, Medical Director
David was externally appointed as new CEO he needed support to set realistic goals; and assure their delivery. We provided 'mission analysis' with an initial Main Effort that saw out of area bed overspill eliminated. The in process feedback was also positive, "Good surfacing of challenges" "Really enjoyable..all on board"
South London and Maudsley
David Bradley & Team, CEO & Execs
"By consolidating the collaborative's scattered data and presenting it in a unique and user-friendly fashion, we now have the tools at our fingertips needed to work with clinicians and system partners to put resources where they will have the biggest impact improve our young people's experience of care and deliver bold but evidence based change"
North West London CAMHS
Richard Lyle, Head of Commissioning & Contracting
"VOT Health have provided unrivalled visibility over our service user journeys and distilled our operating model in ways we didn’t previously appreciate. They are expert at engaging and facilitating our clinicians to adopt new ways of working. Their ‘one team’ approach and close working with my leadership team gives me assurance that changes are locally owned and will sustain"
All Trusts recognise that placing service users Out of Area represents poor care quality because it dislocates the patient from their local care network. It is also high cost, Sheffield Health Partnership (SHPU) was spending many millions on placements classed inappropriate because it could not find space within its own wards. Money that cannot then be spent supporting others in need of care.
We are really pleased to share that SHPU has brought down its OOA bed overspill to zero partnering with VOT. Acute OOA bed usage was averaging over 30beds a year ago. The Trust has been a top-3 OOA inappropriate placement user during 2025, so this represents an enormous improvement in the design and management of its Acute pathway, without compromising patient safety.
CNWL’s COO, Graeme Caul, describes how it achieved long standing OOA placement cessation to HSJ.
Central and North West London utilised our market leading mental health visibility support. As Graeme describes “there is no shortcut to improving acute mental health care. But there is a formula: understand your demand, know your patients, and bring clinical and operational leaders together to act with purpose – every day of the year.” “We began by really understanding our data”
VOT staff developed the pathway visibility local decision makers needed at CNWL to “hold a weekly whole-system event that brings together clinical and operational leaders from across the trust to review data, examine trends, identify delays, and agree on the actions needed to keep the system moving. It’s a model that combines real-time responsiveness with strategic, cross-system insight.”
The annual budget setting cycle is often seen by NHS services as an opportunity to ask for more not less. With funding restricted NHS Trusts must work with a very different mindset.
The Finance Director can get the red pen out to seek to control spend but this approach is not sufficient to sustainably balance the books.
The secret is operationally-led financial improvement.
Read More
The answer isn’t more
Good operations look after the money, it is in the frontline that the vast majority of spend occurs and this is mostly people costs.
All mental health trusts have rapidly increased workforce in recent years. They are typically one of the biggest local employers. You will be surprised then what a small proportion of clinical staff time is spent on direct patient care.
We often run exercises across teams to get staff to detail how time is spent to identify prime opportunities for improvement. By way of example, a home treatment team’s nurses might average 25% at best directly supporting patients face to face or on the phone. The majority is consumed by administration and travel.
Ok, so some administration and travel time is reasonable, but the issue is that staff across the many mental health trusts we’ve worked with don’t know what good looks like; nor are there strong performance controls in place to drive behaviour.
In our home treatment example, staff were only with a patient mid-morning & mid-afternoon as they started and finished at base to plan for the day and access computers to write up notes.
This is a very inefficient use of time, staff recognised that a more modern approach would be to work peripatetically remotely enabled by technology to much increase the ability to see more patients. We were able to increase direct care time by a third.
So, extrapolate this across a Trust. Anyone will tell you how difficult it is to recruit more mental health staff, have you first released the huge gain by using what you’ve got already via a focus on operational rigours?
Community services
PROM measures are still immature and not yet central to decision making. When they are available they can show that the service has not made a significant difference to wellbeing.
Only talking therapies has established recovery targets and linked package of care clarity. This means a mental health trust will have hundreds of staff in community teams that have grown rapidly but not on a firm efficacy and efficiency foundation.
Efficacy measures are absent like step-down recovery rate and trusts are normally poor at combining activity with the workforce that delivered it to understand value for money measures like cost per case.
The focus is largely on contacts per WTE, which has little meaning if the treatment value of the contact is unknown. Contacts will often be just ‘check ins’ particularly when services are ‘holding’ patients because they are risk-averse &/or have no organised themselves to deliver time-limited interventions.
This ‘holding’ common in the likes of a CMHT massively increases cost per case and demands more staff to meet the needs of new referrals.
Wards
Wards too have a similar issue. All mental health trusts are working to ensure purposeful admission in the first instance. You’d be surprised to note that at anytime 1 in 3 or more of inpatients are repeat admitters in the prior 12months, multiple admissions are common. This is containment not treatment.
Ward stays also become extended, adding further to the need for high cost beds. Facilitating early discharge demands close working between ward and community teams especially home treatment. This like 7 day working is still a challenge for most trusts to expedite flow.
Effective financial control
Budget planning is difficult, there is a reason why so many trusts struggle to balance the books, key reasons include:
Forward visibility of funding and need to balance books at a system-level. How do you know a service development today is affordable next year?
Quality will always trump money. A poor CQC report or service user tragedy will trigger a spend response. A senior manager is much more likely to be moved on for a quality over an economy failing, as the former has much more of a hold on the public.
Finance and BI partnership at a service level is not strong. Even when there has been the investment in partners to guide the effective use of resource, this is undermined either because:
the partners are working too remotely from the frontline…and have not built the relationships or understanding of services to challenge clinical and operational leads; or
the underlying data structure and cost centre hierarchies to align workforce and activity is not in place to facilitate value for money insights
Is it any wonder that Finance Directors will look to reserves and unfilled vacancies to balance their books, whilst cost improvement programmes (CIPs) schemes, unloved by clinicians, go undelivered.
There is another way…
Don’t talk about the money
Get it right first time, good process is our friend. We must ensure service models are clear with a focus on removing from process and pathways non value-adding activity.
In a mental health environment this means service models that are:
Time limited
Co-produced around need (not what we can do)
Joined up, so across different teams all can see:
who knows the patient best;
how their need is being met; &
what to do in a crisis
And ensuring process improvement, such as applying Lean methodologies, are a core competency.
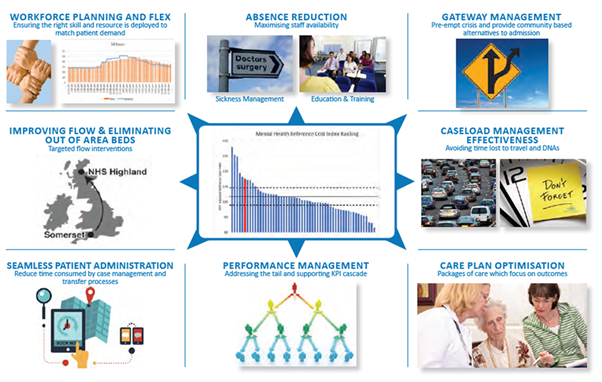
The drivers of efficiency are not hard to list, I call this my mental health ‘wheel of fortune’.
Wheel of fortune
I have already touched on time lost to patient administration or poorly designed process; teams ‘holding’ service users with an absence of time limited intervention is a failure to care plan optimise. The ‘wheel’ additionally includes workforce planning and flex; performance management and absence reduction.
Conversations that focus on doing ‘wheel’ things better will energise clinicians. Money discussions can, however, suck the life out of a room. So our advice is leave CIP quantification to the finance partner to work up offline!
Back office
This leaves corporate areas, which need to lead by example. Just as front line services struggle to record the value they bring to service users, so too back office functions.
I led the NHSI sponsored national Financial Improvement Programme support when paired with Avon & Wiltshire Partnership pre-Covid. The executive team did not shy away from back office savings, sending a clear message by down-sizing and relocating HQ. Whilst importantly recognising the need to invest in the skills to support front line productivity improvement.
What if savings need to be realised at pace?
As any turnaround professional knows you have to grab the cheque book to buy time to reengineer operations. This can be uncomfortable as it requires a command-and-control management style.
Vacancy panels and imposing spend controls, with far more upward delegation is very demanding on an executive team. A necessary evil that no NHS organisation can preserve for long given the friction this generates with clinicians, who unlike a private business are not at risk of redundancy if financial rigour is not maintained.
Conclusion
Quality and economy go hand in hand. To get it right first time a mental health service user needs to experience timely purposeful time limited care.
There cannot be compromise on this, it is an operational model weakness if services are allowed to build a waiting list that then creates the further resource burden associated with waiting list management that reduces staff time available to treat.
Go back to the ‘wheel of fortune’ pick an operational improvement challenge, go from there to optimise value from your workforce and eliminate pressure on budgets.
Trusts don’t give themselves breathing space, it is “one in one out”. It is no surprise that bed usage spills over into out of area from time to time.
There are some obvious things to do to control Acute flow and the rest is culture.
Read More
Containment not treatment
I’ve been working with Mental Health trusts for almost 10 years. What struck me early on was how difficult it was to see care pathways in action. I realised that I was actually looking at a containment not a treatment model.
Staff are understandably risk adverse: they work in silos not understanding what colleagues in other teams are doing; record sharing is often poor, especially between psychiatric liaison and community mental health teams; crisis plans are weak or absent; and when something does go tragically wrong staff fear for their jobs and reputation or are consumed by subsequent investigations. So why take the risk!?
I’ve been told more than once if the patient is on the ward “they are safe, it’s the ones in the community that keep me awake”.
Yet clinicians tell me patients don’t get better on a ward and every admission should be purposeful. Equally, how many times have you read patient accounts of inpatient care, that describe how the process was traumatising, if well intentioned?
So, this is our wicked problem start point.
Obvious things
There are some recurring actions that arise from our flow work with Mental Health trusts. You should explore the following to reduce occupied bed day pressure:
Do you have bed flow grip?
Bed allocations by geographical patch ensure that the bed base is not a buffet; & you need actionable flow metric visibility, e.g. a spike in long stayers will put pressure on beds…so where’s the spike, what’s the resolution & mitigation plan to stay within the bed base?
Do you really have CRHT fidelity?
Your CRHT team should be the virtual ward, is it really only holding at-risk of admission patients? Is it facilitating early discharge and pulling patients from the ward?
Containment over treatment?
What proportion of the Acute bed base is consumed by repeat admitters? You will be surprised, how then are you ensuring that crisis plans are robust and being used to guide staff and psychiatric liaison teams from admitting unnecessarily?
Unnecessary patient moves?
Patient moves restart the treatment clock no matter how well-intended to get a patient closer to home or repatriate from an out of area bed. Typically, one move doubles the spell length of stay.
Culture
Culture is the way we do things around here. So, if you want an organisation that is happy to take positive risk; avoids unnecessary admission; and doesn’t wait for perfection before discharge; my advice would be:
Provide air cover, senior leadership sets behavioural norms. Staff will not take positive risk if they don’t think their seniors have got their backs.
Close the pathway clarity gap. Staff hold onto patients because they don’t know or trust how they will be supported elsewhere in the pathway. Mental health support must be responsive to reduce the risk of crisis presentation and thus pressure on the ward front door. Don’t tolerate waiting lists, ensure services are ‘easy in/easy out’ and the interfaces between them are well understood.
Visibility is key. You must be able to see the extent to which you are delivering orderly step up/step down support to patients. You can then target changes required to meet patient need closer to home with less need for bed days; & importantly assure staff and stakeholders.
But we just don’t have enough beds
We wouldn’t have an out of area problem if we had the acute and step-down beds for our population need, is a common refrain.
Ok, one Trust might have relatively more beds than another, but have you done the obvious and can you hand on heart say you treat and don’t contain?
Conclusion
This is a wicked problem, however, don’t assume it cannot be solved due to a lack of bed capacity.
Studies have repeatedly shown across healthcare settings that the best performers are not those with the most relative resource or the least demand pressure. Take, for example, declining A&E performance. An excellent analysis1 showed that the frequently cited drivers of poor performance of increased attendance, greater complexity and staff shortage were not drivers at all. The driver was a failure to move patients through hospital wards and back home efficiently.
So, if you are going to invest in anything perhaps that should be management capability and process improvement and not the politicians’ answer which always seems to be more front line resource.
1 The A&E crisis: what’s really driving poor performance? Feb-23, Re:State independent think tank